2026 PBC Patient Survey – Result Highlights
The Canadian PBC Society is committed to advocating for people living with PBC. In the spring of 2026, 323 PBC patients from across Canada shared their experience living with PBC
Understanding the PBC patient experience
We need to hear from you! The Canadian PBC Society advocates for PBC patients and while we share much in common, each of us is unique. We are asking 1,200
LYVDELZI® approved for PBC by Health Canada
Gilead Science Inc announced that Health Canada has approved LYVDELZI® (seladelpar) for the treatment of primary biliary cholangitis (PBC) in combination with ursodeoxycholic acid (UDCA) in adults who have had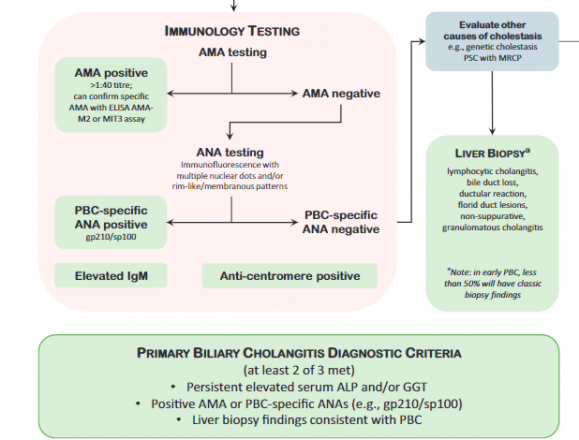
Autoantibodies in Primary Biliary Cholangitis
Learn more about how AMA/ANA is used for PBC diagnosis and risk stratification. This article was published in the November 2022 issue of Clinics in Liver Disease Vol 26 Issue